WHY MANUAL SMALL INCISION CATARACT SURGERY?
WHAT IS MANUAL SMALL INCISION CATARACT SURGERY?
Manual Small Incision Cataract Surgery, also known as MSICS or SICS, is a version of Extracapsular Cataract Extraction (ECCE) cataract surgery.
Unlike ECCE, in which the incision is long and requires multiple sutures, the incision made to the eye in MSICS is much smaller and tunnel-shaped (11 mm vs. 7 mm). This self-sealing “tunnel incision” eliminates the need for sutures, reducing complication risk. Sutures and larger wound size in ECCE result in higher astigmatism, higher probability of infection, and longer recovery times.
MSICS EXPANDS THE SURGEON’S ARSENAL
MSICS provides a logical step forward, not a step backward, and addresses the gap between modern phacoemulsification surgery and management of cataract outliers. Its relevance depends on practice setting or interests, but the international arena is still highly dependent on MSICS as a primary tool for providing affordable cataract surgical care. In certain instances, patient pathology may drive the choice of MSICS.
Examples of patient pathology suitable for MSICS may include advanced pseudoexfoliation, traumatic cataracts, dislocated or subluxated cataracts — genetic or traumatic, hypermature nuclear cataracts, presence of posterior synechia, advanced Fuchs’ dystrophy or other endothelial disease, absence of red reflex, and corneal pathology or previous corneal surgery.
MSICS is recommended for novice learners, with gradual introduction to phacoemulsification.
The complication rates for MSICS and phacoemulsification are comparably low in the hands of experienced surgeons proficient in both techniques. However, MSICS has a much lower surgical complication rate in the hands of trainee surgeons (Haripriya A, Chang DF, Reena M, Shekhar M. Complication rates of phacoemulsification and manual small-incision cataract surgery at Aravind Eye Hospital.
Cataract Refract Surg. 2012 Aug;38(8):1360-9. doi: 10.1016/j.jcrs.2012.04.025. PMID: 22814042).
MORE ABOUT MSICS
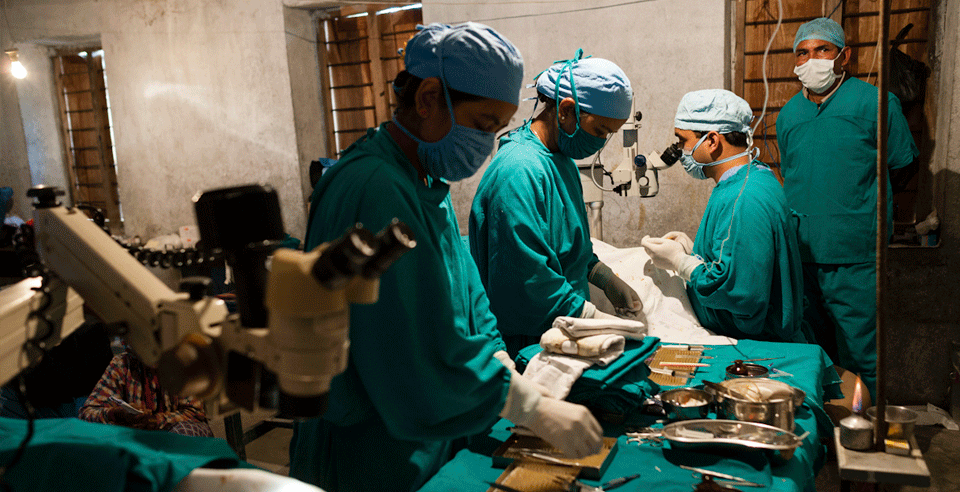
Key surgical care procedure for treating cataract in resource-constrained settings.
MSICS does not require special equipment with a consistent electrical connection. MSICS is usually performed under topical anesthesia. It is preferred when cataracts are harder when cataract-removal surgery has been delayed for years. These characteristics make MSICS especially suited for the delivery of safe and cost-efficient cataract-removal surgery in the resource-constrained clinics of the developing world.
Although MSICS is generally recommended over ECCE among the low-cost procedures, ECCE is still performed in some regions because of the lack of availability of surgeons with MSICS skills. Providing ECCE surgeons with skills in MSICS would benefit many patients in the underserved pockets of the world.
ADVANTAGES OF MANUAL SMALL INCISION CATARACT SURGERY INCLUDE:
- Unlike phacoemulsification, MSICS is a low-cost surgical procedure that does not require expensive equipment.
- It is a high-volume surgery learned in a short span of time.
- It is suitable for all types of cataracts.
- MSICS rehabilitation is quicker with shorter healing times due to the lack of suture-related issues.
- There is less postoperative follow-up with MSICS.
- The learning curve for MSICS is shorter than that for phacoemulsification.

DISADVANTAGES OF MANUAL SMALL INCISION CATARACT SURGERY
- The surgical skill and experience of the surgeon play a significant role in the outcome of an MSICS procedure.
- Excess water discharge from the eye can persist for five to seven days after the surgery.
- Postoperative hyphema, bleeding in the front, internal part of the eye, may occur more often than in other forms of cataract surgery.
- There is mild tenderness in the eye at times due to the scleral incision.
- Surgery-induced astigmatism is higher than in phacoemulsification because the MSICS incision is larger at 6 mm when compared to phacoemulsification at 3.2 mm.

MSICS is usually performed under topical anesthesia. It is preferred when cataracts are harder when cataract removal surgery has been delayed for years. While MSICS is generally recommended over ECCE, ECCE is still performed in many areas
Do you want to know more?
Join our email list for life-changing patient stories who had their sight restored with MSICS and the latest news on HelpMeSee.

Pages
Contact Information
1 Evertrust Plaza, Suite 308
Jersey City, NJ 07302
+1 844-435-7637 (toll-free in the U.S.)
+1 212-221-7606 (international)
For media inquiries, please email us directly at [email protected].
For training inquiries, please email us directly at [email protected].
Tax ID: 27-3207754
![]()
![]()
![]()
![]()
![]()
©2024 HelpMeSee - ALL RIGHTS RESERVED
Privacy & Data Security Policies | Donor Bill of Rights | Financial Disclosure
Training Services Standard Terms and Conditions | General Terms and Conditions of Simulator SBLS Use | Application Data Sharing Consent | HTML Sitemap
HelpMeSee is a 501(c)(3) nonprofit organization registered in the United States.
The HelpMeSee mission is to eradicate preventable cataract blindness globally. We achieve this through an innovative, scalable simulation-based cataract surgical training program. Our program covers Manual Small Incision Cataract Surgery (MSICS), Phacoemulsification Simulation-based Training Course (PSTC), Suturing Simulation-based Training Course (SSTC), Complications Management Course (CMC), Phacoemulsification to MSICS Differences Course (PMDC), and MSICS to Phacoemulsification Differences Course (MPDC). These offerings empower eye care professionals to refine their skills, master vital procedures, and excel in ophthalmology. We are dedicated to restoring vision for those with severe visual impairment and cataract-induced blindness worldwide.
![]()
is a proud recipient of the:

![]()